Recommendation
 based on reviews by Silvio Maltagliati, Florian Chouchou and Jean-Philippe Chaput
based on reviews by Silvio Maltagliati, Florian Chouchou and Jean-Philippe Chaput
Pregnancy has been shown to affect the quality, duration, and pattern of sleep (Paavonen et al., 2017; Reid et al., 2017). These changes have important implications, as insufficient sleep is associated with health problems and complications during labor. In line with studies investigating the general population, a few studies focused on pregnant smokers and have also shown a prevalence of sleep abnormalities (e.g., Danilov et al., 2022; Lange et al., 2018; Paavonen et al., 2017). Studies examining the role of passive smoking on sleep are rare, be it in the general population or in pregnant women.
The aim of the Ciochon et al. study was to investigate the relationship between active or passive smoking and three types of sleep problems during pregnancy: difficulty falling asleep, difficulty staying asleep, and waking up too early. The authors hypothesized that pregnant women's exposure to smoking (active and passive) would increase their risk of sleep problems during pregnancy.
Participants were part of a larger study: the Corona Mums project, which included 3365 pregnant women from Poland, aged 18 to 43 years. These women completed an online questionnaire during the COVID-19 pandemic, from May 2020 to September 2021. The authors conducted multivariate logistic regressions that included the following control variables: socio-demographic, pregnancy-related variables, and psychological variables.
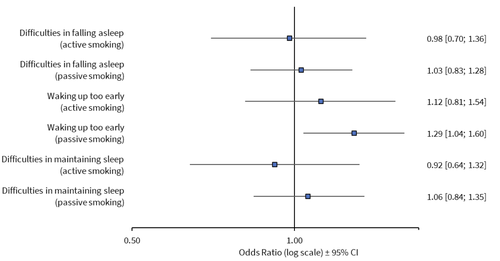
The results of the study showed that passive smoking is a risk factor for waking up too early, but they showed no evidence suggesting that active or passive smoking was related to any of the other sleep variables. The authors highlighted the roles of control variables included in the models. Specifically, sleep difficulties were related to age, place of residence, education, level of anxiety and depression in pregnant women, and the presence of nausea or vomiting. Further, in all the models, the level of anxiety, depression, and trimester of pregnancy (3rd trimester in comparison to 1st and 2nd) were significantly related to the risk of occurrence of sleep problems.
While only one of the six examined associations showed statistical significance, the findings are still useful in highlighting potential risks associated with passive smoking and sleep disturbances during pregnancy. The study also underscores the need for more comprehensive investigations, including direct measures of sleep quality, such as actigraphy or polysomnography, which are necessary to better understand the underlying mechanisms and to confirm the potential impacts of both active and passive smoking on sleep during pregnancy.
DOI or URL of the preprint: https://doi.org/10.5281/zenodo.14048004
Version of the preprint: 2
, posted 14 Jan 2025, validated 14 Jan 2025We would like to thank the authors for their tremendous work in responding to the reviewers' comments. This has improved the article, which already had several strengths.
However, one reviewer highlighted some remaining issues, and I agree with him. The reviewer also indicated ways to respond to his comments. If the authors decide to respond to the latter, I will be pleased to review the article again.
, 14 Jan 2025I have carefully reviewed the authors' point-by-point responses to my comments and appreciate the effort they have put into addressing them. However, I still have major concerns that remain to be addressed.
- Absence of evidence is not evidence of absence (e.g., Alderson, 2004). On several occasions in the manuscript, the authors confuse the absence of statistical evidence (p > .05) with the absence of an effect (which would require an equivalence test or a Bayesian approach to be demonstrated).
For example: ‘Interestingly, active smoking was not associated with sleep difficulties.’ should read ‘Results showed no evidence of an association between active smoking and sleep difficulties.’ Please adjust the manuscript throughout.
- The abstract states that passive smoking affects sleep. But in fact, this effect is only observed in one sleep variable out of three. Please be more specific in the abstract.
“The incidence of sleep problems in pregnant women was shown to be associated with exposure to cigarette smoke (passive smoking), while controlling for a range of individual variables (age, education, place of residence, satisfaction with the woman's life, and economic situation, pregnancy complications, levels of state anxiety and depressive symptoms, trimester of pregnancy, nausea or vomiting during pregnancy, and COVID-19 infections)’ could read ‘Passive smoking was associated with one of the three variables used to assess sleep problems (i.e., waking up early).’
- The term ‘stimulant’ is often used to define the smoking variable, but the actual measure is smoking. There is not measure of the concentration of stimulant in the study.
For example: ‘Each aspect of sleep difficulties and stimulant use’, ‘Sleep problems and stimulants use assessment’. Please reword throughout the manuscript.
- The term ‘incidence’ does not seem appropriate as there seem to be a single measurement period. Therefore, it would be difficult to assert whether these are new or pre-existing cases. The term prevalence may be more appropriate. That being said, using ‘sleep problems’ may work as well (no mention of incidence or prevalence).
- I agree with the Recommender’s suggestion to add a Figure and recommend adding at least one figure or a panel of several figures as figures are always useful for the readers to clarify the results. For example, a figure including the 6 ORs of passive and active smoking the 3 sleep variables, with a note to say that these results come from different models and are aggregated in a single figure for clearer illustration purposes.
- In Table 1, the asterisks are not needed. The footnote is sufficient.
- I am still a bit hesitant regarding the interpretation of the findings and their links with previous literature. Indeed, authors state that "their results are consistent with those obtained by other researchers". However, if I am correct, previous research focused on active smoking, not passive smoking. As such, I wonder whether we can say that these results are actually consistent. Could authors please check that the Discussion section closely follow their findings?
- I suggest adding a ‘Limitations’ section. Among other points, I suggest adding two limitations: The sleep variables are open to interpretation (e.g., too early; ‘maintain sleep’) and could therefore be more accurate. Since 3 variables were used to test for sleep problems and address the same research question, a conservative statistical approach to reduce the risk of type 1 errors would be to correct for the number of partial tests (n = 3) (Bonferroni correction), reducing the significance threshold to .05/3 = .016. Such correction would make the association between passive smoking and weaking up early non-significant).
Reference:
- Alderson P. Absence of evidence is not evidence of absence. BMJ. 2004;328(7438):476–477. https://doi.org/10.1136/bmj.328.7438.476
Most of my comments have been addressed, particularly in the discussion
, 13 Nov 2024Thank you for revising the manuscript based on the feedback received. I think the authors adequately addressed the comments raised in their revised paper and I have nothing further to suggest. I feel the paper can be accepted.
DOI or URL of the preprint: https://doi.org/10.5281/zenodo.11383758
Version of the preprint: 1
The final version was published on the preprint server.
https://doi.org/10.5281/zenodo.14048004
, posted 12 Aug 2024, validated 13 Aug 2024I would like to thank the authors for the submission of their article "Cigarette smoke exposure as a potential risk factor for sleep problems in pregnant women" and congratulate them on the work carried out for this article.
The aim of the article is to investigate the relationship between active or passive smoking and the onset of three types of sleep problems (i.e. difficulty falling asleep, maintaining sleep and waking up too early) during pregnancy. The authors hypothesized that pregnant women's exposure to nicotine (active and passive) will increase their risk of sleep problems during pregnancy.
Participants were part of a larger study :Corona Mums project. This study included 3365 pregnant women from different parts of Poland, aged 18 to 43 years (M = 30.7, SD = 3.87) who completed an online questionnaire during the covid-19 pandemy. The authors perfomed multivariate logistic regression that included control variables (i.e., socio-demographic, related to pregnancy, and psychological variables)
The authors found that passive smoking is a risk factor for waking up too early but active smoking was not related to any of the sleep problems investigated. However, authors highlighted the roles of the control varibles included in the models performed.
All three reviewers found the article interesting and well-written. I agree with them. They also posed a number of questions that need to be answered and expressed a few concerns that need to be resolved before I can recommend the article.
All their comments are in the document(s) attached. In sum, 3 sections particularly need to be revised
The background needs to be reinforced (e.g. explicitly state the added value of the article, explain and/or discuss the particular context of covid).
Methods need to be clarified (e.g. choice of questionnaire, variables, duration or dates of data collection) and alternative or complementary analyses were proposed.
The discussion section needs more explanation of the results, a section devoted explicitly to strengths and limitations could be written, and the conclusion needs to be revised.
I had some comments and questions (on my own) to add to their reviews :
The authors highlighted the possible bias due to the stimatization of pregnant women who smoke during pregnancy. This is an important point. What about the "discret way" (less visible) to have the daily nicotine dose (patch, gum...)? The women could have stop smoking but still be expose directly to nicotine
The difference between before and during the pregnancy can be discuss for some variables. For instance : the smoking cessation (because of the health problem, or the social pressure) was not investigate or discuss. Did some of the pregnant women used to smoke before pregnancy? Did this cessation increase stress, sleep problem? The fact that the women had contracted the covid before or during the pregnancy, or before and during the pregnancy (so, at least twice), could have different impact.
The authors stated that the research followed the guideline of the bioethics committee. However it is not clear for me if this particular study obtain an ethic committee agreement.
The coding of "trimester of pregnancy" (LL 200-201) is not clear for me.
I wonder how missing data were managed.
The article also contain some typos (e.g., foetus or fetus : both appear in the article, L102 the brackets)
Finally, is it possible to add a figure that illustrate your results?
Some of these articles (not exhaustive) may be helpful https://jcsm.aasm.org/doi/pdf/10.5664/jcsm.8930
https://onlinelibrary.wiley.com/doi/pdfdirect/10.1111/jsr.13432
https://www.thelancet.com/pdfs/journals/eclinm/PIIS2589-5370(21)00196-6.pdf
https://doi.org/10.1016/j.pec.2020.09.031
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7295479/
Thank you again for submitting your article to PCI health and movement science. I hope these comments will be useful
, 11 Jun 2024Overview and general recommendation:
Thank you for giving me this opportunity to read this interesting manuscript. I have a few comments and I hope they will help to improve the overall quality of the article.
Introduction:
I have the feeling that the Introduction section is pretty straightforward and nicely introduces the aim of the study.
Methods and results:
1- I think it would be worthwhile to add the references that were used to create the administered questionnaires. Were they validated by previous studies? What were the exact questions? Thank you very much. If the scales were not validated, it should be at the very least mentioned as a limitation in the Discussion section.
2- What does “city100,000 =1” refer to? Could authors please clarify this point in the main text (as done in Table 1) ?
3- Just a point of curiosity: have authors considered combining active and passive smoking together? So, we would get four categories: “active + passive smoking” ; “active smoking only” ; “passive smoking only” and “neither active nor passive smoking”.
4- Were variables scaled and mean-centered before computing logistics regressions?
5- I am not an expert in these analyses, but I don’t think that odds ratios can be interpreted as a percentage of reduction in risks (see Norton et al., 2018, JAMA, 10.1001/jama.2018.6971 for example). Could authors please clarify their interpretation of odds ratio?
6- I would be curious to examine the univariate associations between smoking status and sleep patterns. For example, it is possible that depression or anxiety could mediate (and blur) the association between smoking status and sleep (e.g., smoking depression sleep problems). Maybe that these univariate associations could be displayed in Table 1?
Discussion :
1- I have the feeling that results should be discussed with a bit more caution in some parts of the Discussion section. For example, the sentence “Similarly, in our study, we found that women in the 3rd trimester reported 2 - 3 times higher occurrence of sleep problems, than women in earlier stages of pregnancy” does not echo the findings of Danilov et al., (2020) that focused on the links between smoking status and sleep, at different stages of pregnancy.
In the same perspective, the conclusions that are drawn from the study should be tempered: for example, “we suggest that nicotine exposure during pregnancy might have a potentially detrimental impact on a mother's sleep quality”. Regarding high rates of Type 1 errors due to multiple tests and with a single significant association (without applying false discovery rate methods), I don’t think that the evidence is strong enough to support this claim. Maybe authors could consider rephrasing this type of sentences?
2- As nicely introduced (Lines 392-394), it could be relevant to examine the correlates of smoking status? Maybe authors could consider adding a correlation table between smoking status and demographic/psychological variables?
3- The only significant association is between passive smoking and waking up too early. I struggle to understand why this significant association emerged for passive smoking, not for active smoking? And why it emerged only on this indicator of sleep patterns. I think that power issues partly account for the non-significant associations, but a more in-depth discussion of these results would be welcome. Thank you.
4- I think that limitations of the previous study would deserve to be mentioned in the Discussion section: self-reported nature of the data, lack of adjustment for important covariates (e.g., physical activity, food-related behaviors), cross-sectional nature of the data.
I wish the best of luck to the authors for their ongoing projects.
Silvio Maltagliati
Ciochon and colleagues propose an interesting study on risk factors for sleep problems in pregnant women. They examined cigarette smoke exposure through an online survey conducted during the COVID-19 pandemic, involving 3,365 Polish adult women. Their findings revealed a higher independent risk for sleep problems associated with passive smoking, but not with active smoking. They utilized logistic multivariate analysis for this study. However, several issues undermine these results:
Major comments
· What is the added value of the article to the existing literature? Previous studies have shown the increased risk in pregnant women. What new insights do these findings provide? Specifically, how can the absence of an effect for active smoking be explained?
· The questionnaires regarding sleep pose a problem: only three binary (yes/no) questions about sleep were used, leading to coarse response sampling – is this why there was a lack of responses from smokers? Other validated questionnaires exist in the literature. Why were they not used? Have other studies used or validated the sleep questions you used? This point should at least be addressed in the limitations section.
· Sleep disorders exist even in the absence of pregnancy. The lack of a control group does not allow for a real estimation of the disorders. This point should also be addressed in the limitations section.
· In the analyses, segmenting into three different analyses excludes the exploration of the most severe profiles: those who accumulate all three types of sleep disturbances. I recommend constructing profiles with 3 sleep disturbances, then 2, then 1.
· A large part of the analyses in the results section does not relate to the objectives. These parts should be removed or significantly reduced.
· Caution, the results do not support the conclusion: nothing in this work allows us to say that nicotine is at play here.
· For the variables of interest (smoking), an initial step with univariate models would be informative, followed by a complete model.
· Other variables should be included in the model: chronic diseases: gestational diabetes, hypertension, etc.
· The particular context of COVID-19 should be discussed in more detail: it is not an ordinary context.
· As you point out in the text, the quality and quantity of sleep are two elements related to health and vulnerability. There is no exploration of sleep duration (number of hours) and its quality (e.g., "I slept well"). These points should be discussed in the limitations section at a minimum.
Minor comments
· The references are not always relevant: Lester 2013 does not include sleep in Maslow's hierarchy.
· Missing definition of passive smoking exposure.
· Lack of references: lines 62, 83, 114.
· Introduction: Sleep problems also affect men.
· Incorrect reference: line 120 is not relevant.
· The percentages presented in the results need to be explained in the methods.
· The names of the models (1, 2) should also be explained.
Responses to PCI questions
-Does the title clearly reflect the content of the article?
Yes
-Does the abstract present the main findings of the study?
Yes
-Are the research questions/hypotheses/predictions clearly presented?
No. No differentiation between the hypotheses of active and passive exposures.
-Does the introduction build on relevant research in the field?
No. The introduction is rich in references but a bit long and confusing, and it does not present the interest of the study here.
-Are the methods and analyses sufficiently detailed to allow replication by other researchers?
Yes
-Are the methods and statistical analyses appropriate and well described?
Yes
-In the case of negative results, is there a statistical power analysis (or an adequate Bayesian analysis or equivalence testing)?
No. The most vulnerable profiles are not studied here.
Are the results described and interpreted correctly?
Yes
-Have the authors appropriately emphasized the strengths and limitations of their study/theory/methods/argument?
No. Several limitations are not presented.
-Are the conclusions adequately supported by the results (without overstating the implications of the findings)?
No, not the last conclusion.
, 19 Jun 2024This paper examines whether cigarette smoke exposure is a risk factor for sleep problems in pregnant women. The authors found that passive smoking is a risk factor for sleep problems in pregnant women, especially in the aspect of waking up too early. However, active smoking was not related to sleep problems. The paper is interesting and well-written. However, some aspects need to be clarified.
Abstract: The study design (i.e. cross-sectional) should be indicated. Years and months of data collection should also be mentioned.
Introduction: Good section but quite long. Introduction sections should be concise and typically include 5 key things: (1) the problem; (2) what we know on the topic (existing evidence); (3) what this study adds (originality); (4) objective; and (5) hypothesis. I feel that point 3 is a bit missing. Authors should make the knowledge gaps more obvious and tell the readers how the present study will address them (i.e. incremental knowledge).
Methods: It’s not clear if the sample is a convenience sample of pregnant women or a random sample. This has implications for possible biases and external validity. Lines 172-176 are about the Results, not the Methods. This text should be moved to the Results section. With regard to the 3 sleep questions, have they been validated?
Results: Please report only 2 decimals for the ORs and 95% CIs.
Discussion: A paragraph highlighting the main limitations of this study should be included before the conclusions. Furthermore, the authors are encouraged to provide an explanation or at least speculate on the odd finding observed, i.e. that only passive smoking and not active smoking was associated with sleep problems in pregnant women.
