Recommendation
 based on reviews by Paquito Bernard and 1 anonymous reviewer
based on reviews by Paquito Bernard and 1 anonymous reviewer
This article (Goubran et al., 2024) presents a comprehensive systematic review and meta-analysis examining the relationship between kinesiophobia and physical activity. The inclusion of multiple health conditions and diverse measures of physical activity and kinesiophobia provides a broad perspective on the issue.
Kinesiophobia (i.e., an excessive, irrational, and debilitating fear of movement) is thought to contribute to negative affective associations towards physical activity and avoidance behaviors, leading to decreased engagement in physical activity. Thus, the relationship between kinesiophobia and physical activity merits further investigation, particularly in health conditions where physical activity has a preventative and/or therapeutic role.
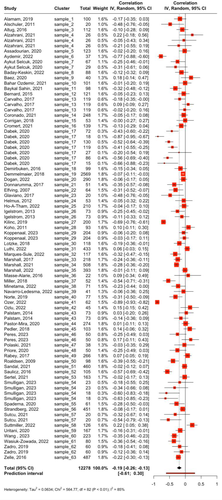
The results of this meta-analysis (k = 83, n = 12,278) indicate a small-to-moderate negative correlation between kinesiophobia and physical activity (r = −0.19; 95% CI: −0.26 to −0.13; I2 = 85.5%; p < 0.0001.) Substantial heterogeneity and publication bias were noted, but p-curve analysis suggested true effects. Notably, this finding was consistent across studies using both self-report and objective device-based measures, and there was no evidence of a moderating effect of different measurement instruments or physical activity outcomes.
Subgroup analyses revealed that the negative association between kinesiophobia and physical activity is significant in patients with cardiac, rheumatologic, neurologic, or pulmonary conditions but not in those with chronic or acute pain. This latter finding underscores the need to distinguish kinesiophobia from pain. Understanding that the fear of pain, injury, or aggravating an underlying condition, rather than actual pain, is associated with physical inactivity is important to consider when developing interventions to promote physical activity. Tailored interventions that address kinesiophobia specific to different health conditions could enhance physical activity levels and improve health outcomes. Further research is needed to explore the mechanisms underlying kinesiophobia and evaluate the efficacy of targeted interventions to mitigate its impact.
This article makes an important contribution to our understanding of the relationship between kinesiophobia and physical activity. It provides evidence that fear of movement can be a barrier to physical activity in certain health conditions and highlights the need for condition-specific approaches to address this issue. This work is highly relevant for clinicians, researchers, and public health policymakers aiming to improve physical activity levels and overall health outcomes in a variety of populations.
References
Goubran, M., Farajzadeh, A., Lahart, I.M., Bilodeau, M. & Boisgontier, M.P. (2024). Physical activity and kinesiophobia: A systematic review and meta-analysis. MedRxiv, version. 3 peer-reviewed and recommended by Peer Community in Health and Movement Science. https://doi.org/10.1101/2023.08.17.23294240
, 12 Jun 2024Authors did a serious, rigorous job with this second version. The updated methodological approach (i.e., contact with authors, various key words, multilevel meta-analyses, and sensitivity analyses) is exemplar. The discussion section is short but instructive. A no significant association between physical activity and kinesiophobia among people with chronic pain was a surprising finding. However, this result is well explained in the discussion.
I tested the R code (wrong link in the preprint), everything seems ok . I obtained the same findings, but I did not find the code associated with the "prediction interval".
The shared data is a very good solution for a future update of this well-structured meta-analysis.
DOI or URL of the preprint: https://doi.org/10.1101/2023.08.17.23294240
Version of the preprint: 1
Date: May 3, 2024
Manuscript Title: Physical Activity and Kinesiophobia: A Systematic Review and Meta-Analysis
Manuscript ID: PCI HMS 39
Dear Recommender,
We would like to thank the reviewers for the provision of valuable comments that contributed to improve the quality of our manuscript titled “Physical Activity and Kinesiophobia: A Systematic Review and Meta-Analysis”.
Please find below our point-by-point responses to their comments. The reviewer’s comments are in bold, our responses are in regular font, and quotes from the manuscript are in italics.
Best regards,
Matthieu Boisgontier
---
REVIEWER 1
---
Reviewer 1: In the present study, the authors examined the associations between kinesiophobia and physical activity outcomes in adults. In my opinion the authors address a relevant question. However, I have highlighted some limitations which dampen my enthusiasm for the manuscript. My greatest concerns with this work were the methodological weaknesses. Author did a great job (thorough analyses, very good graphic representation, sensitivity analyses, data/code sharing) but this review may not be ‘systematic’. Following are some comments based on questions or concerns that arose in my reading. I hope they are useful to the authors.
Authors: The authors are thankful to Reviewer 1 for the critical and constructive evaluation of our work.
Reviewer 1 (Introduction): In my perspective, this section should be revised. Indeed, kinesiophobia is presented as an interpersonal determinant of physical activity. However, it’s a PA determinant ‘only’ for people with injuries, chronic pain, fatigue, or illness. In other words, it’s an important factor in clinical context.
Authors: We agree that kinesiophobia is an important factor in a clinical context, which is consistent with our presentation of kinesiophobia as an intrapersonal (not interpersonal) determinant of physical activity.
Page 4, line 63: “Another intrapersonal factor of interest is kinesiophobia, […].”
Authors: As recommended, we now emphasize the importance of physical activity in clinical contexts:
Page 1, lines 15-16: “Physical activity contributes to the primary, secondary, and tertiary prevention of multiple diseases.”
Page 4, lines 55-58: “Physical activity also plays an important role in secondary and tertiary prevention by reducing the impact, slowing the progression, and preventing the recurrence of multiple conditions, including cardiovascular disease (11,12), osteoarthritis (13), stroke (14,15), and cancer (16).”
Authors: However, kinesiophobia is not necessarily tied to a clinical or pain condition. The presence of kinesiophobia in otherwise healthy adults is also possible (e.g., Bahar Ozdemir, 2021), due to the irrational nature of this phobia. This irrationality can be captured by TSK questions such as “I can’t do all the things normal people do because it’s too easy for me to get injured”, “My body is telling me I have something dangerously wrong”, “I am afraid that I might injure myself accidentally”, or “I’m afraid that I might injury myself if I exercise”. The “sense of vulnerability” that defines kinesiophobia is not necessarily related to an actual pain, injury, or medical condition. This point is now clarified in the manuscript.
Page 5, lines 68-70: “While kinesiophobia is often observed in the context of pain or a clinical condition, its presence in otherwise healthy adults is also possible (29) due to the irrational nature of this phobic condition.”
Reviewer 1 (Introduction): Authors suggested that kinesiophobia has a major role in dual models. This paragraph could be shortened because kinesiophobia is not a major component of these models.
Authors: As suggested, this paragraph has been shortened. The purpose of this section is to position our study in a theoretical framework.
Page 5, lines 73-82: “The relationship between kinesiophobia and physical activity can be explained by theories suggesting that the perception of a cue related to physical activity automatically activates the concept of physical activity as well as the unpleasant (or pleasant) affective memories associated with this concept (32-35). This activation results in an impulse that favors the tendency to avoid (or approach) physical activity (36). Thus, negative affective associations are likely to hinder physical activity. Accordingly, an aversive fear of pain, injury, or aggravation of a medical condition that has been associated with the concept of movement may result in the development of automatic avoidance behaviors that contribute to the maintenance and exacerbation of this fear, and ultimately lead to a phobic state (i.e., kinesiophobia) that diminishes the ability to engage in regular physical activity.”
Reviewer 1 (Introduction): Previous literature reviews about kinesiophobia should be presented.
Authors: As recommended, previous literature reviews related to kinesiophobia and physical activity have been included in the Introduction section.
Page 4, lines 83-88: “Previous systematic syntheses of the literature on this topic include a meta-analysis (37) and two systematic reviews (38,39). The main results or these reviews suggest that exercise interventions may reduce kinesiophobia in individuals with back pain. While back pain is one condition that may contribute to kinesiophobia, it is not the only one. The relationship between physical activity and kinesiophobia should be investigated in other conditions such as cardiac, neurological, and rheumatologic conditions.”
Reviewer 1 (Introduction): Also, the factors tested in the meta-regressions (age, women, pain) should be substantiated in this section.
Authors: We have now clarified that these meta-regressions are exploratory and references supporting these analyses have been added.
Page 6, lines 96-97: “Finally, Finally, because kinesiophobia and physical activity can vary with age, sex, and pain (40,41), we explored the influence of these factors on the association between kinesiophobia and physical activity.”
Reviewer 1 (Methods): There is an essential limit with the current search strategy. Authors focused exclusively on the “kinesiophobia” word. It is an adapted strategy to identify the studies using TSK. However, the investigations collecting data with the Fear-Avoidance Belief Questionnaire (FABQ) can be published without the kinesiophobia word. After a quick search with FABQ and physical activity’, I identified several not included papers. PA self-reported questionnaires: doi:10.3205/psm000057, doi:10.1371/journal.pone.0193566, doi:10.1002/acr.23419, doi:10.1371/journal.pone.0276974, doi:10.1016/j.ptsp.2017.07.002
Authors: We fully agree that our search strategy was too narrow, and we are grateful to Reviewer 1 for pointing this out so that we could conduct a more thorough review of the literature. The five studies mentioned by the reviewer were identified by the new search strategy. One of them reported a Pearson’s r correlation value (Glaviano et al., 2017), one of them reported a Spearman’s rho correlation value (Leonhardt et al., 2009), two provided enough information to compute the r value (Demmelmaier et al., 2018; Ho-A-Tham et al., 2022), and one of them was not included because the article did not provide enough information and we did not receive a response to the data request we emailed (Alodaibi et al., 2018).
Reviewer 1 (Methods): Authors should update their search strategy with more representative key words (e.g., with the name of validated questionnaires). Also, the references of this review should be explored (Effects of Exercise Training on Fear-Avoidance in Pain and Pain-Free Populations: Systematic Review and Meta-analysis). Data collected before the exercise intervention may be useful. Also, physical activity synonyms (e.g., walking) should be added in the search strategy for CINAHL and Psychinfo. In my perspective, SPORTDISCUS database should also be explored.
Authors: The search strategy has been modified according to these recommendations.
Page 6, lines 102-111: “Potential studies were identified by searching the MEDLINE (via PubMed), PsychInfo, CINAHL, EMBASE, and SPORTDiscus databases. In October 2023, two reviewers (MG and AF) searched for all available records using the following combination of keywords in the title or abstract of the article: (“kinesiophobia” OR “fear avoidance” OR “fear of movement” OR “movement phobia” OR “movement fear”) AND (“physical activity” OR “exercise” OR “walking”). In PsychInfo the limits “clinical trial”, “quantitative study”, “peer-reviewed journal”, “English”, and “human” were used. In PubMed the limits “clinical trial”, “observational study”, “RCT”, “English” were used. In SPORTDiscus the limits “peer-reviewed”, “English”, “academic journal”, and “article” were used. In CINAHL the limits “peer-reviewed”, “English”, “research article”, “journal article”, and “humans” were used.”
Reviewer 1 (Methods): I don’t understand the following methodological choice: “When a study measured physical activity with both a questionnaire and accelerometers, the correlation included in the analysis was that of the most reliable outcome, i.e., the accelerometer-based outcome.” Associations examined in a same study can be included in a multilevel meta-analysis. Furthermore, a meta-analysis is carried out for PA self-reported measures in your manuscript. Thus, 5 studies are missing in this analysis.
Authors: We used the ‘metafor’ R package to compare the performance of our 2-level meta-analysis to the 3-level meta-analysis suggested by Reviewer 1. Results supported the reviewer’s suggestion. Therefore, our results are now based on 3-level models.
Page 9, lines 172-176: “Correlation estimates were nested within studies using the ‘cluster’ argument to account for the dependencies between these estimates, resulting in a three-level meta-analysis (level 1: participants, level 2: correlation estimates, level 3: studies). The distribution of variance across levels was assessed using the multilevel version of I2 (54). The performance of the 2-level and 3-level meta-analyses was assessed and compared using the {metafor} R package (51,52).”
Page 6, lines 376-381: “The 3-level model showed a better fit than the 2-level model with lower Akaike’s 's information criterion (AIC) (28.4 vs. 39.0) and Bayesian information criterion (BIC) (35.6 vs. 43.8), indicating better performance. These lower AIC and BIC are consistent with the significant likelihood ratio test (LRT) comparing the two models (χ2 = 12.67, p = 0.0004). Therefore, although the 3-level model introduces an additional parameter, this added complexity has improved our estimate of the pooled effect.”
Reviewer 1 (Methods): Could you provide more details about this inclusion criterion: “formally test the association between these two variables”. Did you include the studies reporting only an univariate AND OR multivariate association (e.g., beta) (see Meta Essentials to manage them [Suurmond R, van Rhee H, Hak T.]).
Authors: As recommended, we have now clarified that one of the inclusion criteria was that the study formally tested the association between kinesiophobia and physical activity, irrespective of the nature of the association. Only one article that reported a beta value did not report a univariate correlation value (Huijnen et al., 2010). However, the information provided in this article was not sufficient to compute the r value and we did not receive a response to our data request. The result of this article is presented in the Descriptive Results section.
Page 7, lines 118-119: “[…] and formally test the association between these two variables, be it a univariate or multivariate test.”
Page 17, lines 344-347: “The remaining study did not report a correlation coefficient and was therefore not included in the meta-analysis (117). This study reported a non-statistically significant positive association between physical activity and kinesiophobia based on a standardized beta coefficient.”
Reviewer 1 (Methods): The current review has been preregistered in Prospero. It is a good point. However, meta-analyses were not planed (e.g., “We do not plan on doing an analysis of subgroups or subsets”) and Risk of bias (quality) assessments were not the tool presented in the manuscript. These gaps should be explained in the current manuscript.
Authors: The meta-analysis was not pre-registered because the author with this expertise joined only after the systematic review was conducted.
Page 24, lines 514-521: “The meta-analysis was not pre-registered because the author with this expertise (IML) joined only after the systematic review was conducted. However, since the pre-registered systematic review defines the studies included in the meta-analysis and since the {meta} R package (50) provides very few degrees of freedom, there was little room for bias in the main and secondary meta-analyses. This reasoning also applies for the subgroup analyses as the health conditions, types of physical activity measures, measurement instruments, and outcomes, as well as the kinesiophobia measurement instruments were imposed by the studies that were included in the systematic review.”
Authors: The pre-registered quality assessments (TREND and CONSORT) are now used in the manuscript.
Page 8, lines 154-159: “The risk of bias of the studies included in the systematic review was estimated using the National Institutes of Health (NIH) Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies (46), the Transparent Reporting of Evaluations with Non-Randomized Designs (TREND) reporting checklist (47), and the Consolidated Standards of Reporting Trials (CONSORT) reporting checklist for randomized trials (48). All scores were normalized to a 0-10 scale to make them comparable across assessment instruments (Table 1).”
Reviewer 1 (Methods): The risk of bias was characterized with the critical appraisal tool for assessing the quality of cross-sectional studies (AXIS). However, there are several randomized controlled trials among included studies (e.g., Priore 2020). They should be assessed with a more specific tool. Additionally, detailed findings for each study should be provided in supplementary files.
Authors: As recommended, we now use a specific tool for each type of study and the detailed findings have been added to the Zenodo repository.
Page 8, lines 153-158: “The risk of bias of the studies included in the systematic review was estimated using the National Institutes of Health (NIH) Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies (44), the Transparent Reporting of Evaluations with Non-Randomized Designs (TREND) reporting checklist (45), and the Consolidated Standards of Reporting Trials (CONSORT) reporting checklist for randomized trials (46). All scores were normalized to a 0-10 scale to make them comparable across assessment instruments (Table 1).”
Reviewer 1 (Results): There is a mistake about the I2 in abstract (I2 = 91.8%).
Authors: The I2 in the abstract has been updated according to the results of the 3-level meta-analysis (I2 = 85.5%).
Reviewer 1 (Results): The study design and context of assessment (e.g., clinical, online...) of included investigations should be added in Table 2.
Authors: As recommended, study design and context of assessment have been added to Table 1.
Reviewer 1 (Results): “The remaining 10 authors did not respond to our email.” Authors should provide the references of these 10 papers in supplementary file. As reviewer, I can’t know if you “miss” a paper or authors did not share their data/findings (e.g., doi: 10.2340/16501977-1927).
Authors: The reference of the articles whose authors did not respond to our email have been added.
Page 13, lines 248-249: “Seventeen emails remained unanswered (92-103,105,106,108-110).”
Reviewer 1 (Methods): The global bias-corrected estimate should be also presented in the abstract and added in the table 2.
Authors: Thanks to the modification suggested by Reviewer 1, the analyses are now based on three-level models, which have shown superior performance compared to the two-level models we used previously. However, Rücker’s limit meta-analysis method, which was used to compute a bias-corrected estimate of the true effect size in the previous version of the manuscript, is not implemented for 3-level meta-analyses. We also tried other functions for bias correction, such as the trimfill() and the copas(), but they were also not implemented for these models. However, the abstract now clearly mentions the evidence for publication bias.
Page 2, lines 29-30: “Funnel plot analysis showed evidence of publication bias, but p-curve analysis suggested that our results could not be caused by selective reporting.”
Reviewer 1 (Limits): Kinesophobia is a dynamic psychological variable. Physical exercise interventions or cognitive behavioral therapy can decrease the kinesophobia level. However, you did not “control” the time of assessment. It should be highlighted in Limits.
Authors: This potential limitation is now mentioned in the manuscript.
Page 24, lines 509-512: “Because kinesiophobia is a state, i.e., a dynamic psychological variable, the time difference between the physical activity and kinesiophobia assessments, as well as the context of assessment, may have influenced the results.”
Reviewer 1 (Limits): TSK scales have been criticized because different factor models exist between them (DOI: 10.3109/09593980802662160). These structural differences may influence the findings of the current work.
Authors: This potential limitation is now mentioned in the manuscript.
Page 24, lines 512-514: “While a subgroup meta-analysis showed no evidence of an effect of the type of TSK scale, inconsistencies have been noted in the purported dimensions assessed by different TSK scales or across populations (197), which may have influenced our results.”
Reviewer 1 (Limits): The question-behavior effect (DOI: 10.1037/hea0000104) could underestimate the association between kinesiophobia and PA.
Authors: The question-behavior effect refers to the phenomenon that asking individuals about a behavior increases the likelihood that they will engage in that behavior. Because most of our studies were cross-sectional and, when they were not, the data were collected at a single point in time (i.e., at baseline), we are not sure how the question-behavior effect might have affected our results. We therefore decided not to mention it in our manuscript.
---
REVIEWER 2
---
I applaud the authors for their rigorous analysis of such an important research topic, which aims to systematically look at the role of fear and aversion of movement on subjective and objective measures of physical activity behavior. I am tempted to accept it as it is; however, I have some major comments for the authors to think about, and a few minor ones as well.
Authors: The authors are thankful to Reviewer 2 for the positive evaluation of our work.
Reviewer 2 (Introduction): First, it is true that these data are highly relevant for dual-process models, which are very popular at this time (example: ART of PA theory). However, they are also highly relevant for other models, such as the Affective Health Behavior Framework (AHBF) (Williams & Evans, 2014; Stevens et al., 2020) and the WANT model of physical activity and sedentarism motivation (Stults-Kolehmainen, et al., 2020). [Note: Dual process models are simply called “dual models” by the authors at least once in the manuscript.]
- Williams, D. M., & Evans, D. R. (2014). Current emotion research in health behavior science. Emotion Review, 6(3), 277-287.
- Stevens, C. J., Baldwin, A. S., Bryan, A. D., Conner, M., Rhodes, R. E., & Williams, D. M. (2020). Affective determinants of physical activity: a conceptual framework and narrative review. Frontiers in Psychology, 3366.
- Stults-Kolehmainen, M. A., Blacutt, M., Bartholomew, J. B., Gilson, T. A., Ash, G. I., McKee, P. C., & Sinha, R. (2020). Motivation states for physical activity and sedentary behavior: desire, urge, wanting, and craving. Frontiers in Psychology, 11, 568390.
Authors: As recommended, other models for which our data can be relevant have been added to the Introduction section.
Page 5, lines 70-72: “The irrational fear that characterizes kinesiophobia is likely to influence the desires and impulses for movement and rest (Stults-Kolehmainen et al., 2020), as well as affective determinants of physical activity in general (Stevens et al. 2020).”
Reviewer 2 (Results): There seems to be some unexplored temporal issues in the methodologies examined. For instance, the self-report measures are all retrospective (correct?). Were studies looking at PA, that was assessed retrospectively, with measures of Kinesiophobia taken at the same time? Where there any prospective studies with these measures? With objective measures, was the Kinesiophobia measure assessed at the beginning or end? Some measures look at PA that was assessed, perhaps, over a week, two weeks or a month. Do you think this makes any difference? In other words, there could be some influence of memory and reaction to measures of kinesiophobia.
Authors: The temporal information mentioned by Reviewer 2 has now been included in the Descriptive Results section. Given that most studies used similar methods in terms of temporal information, we do not think these variables are critical for our study.
Page 16, lines 317-323: “These devices were worn for 5 days (n = 1), 6 days (n = 1), 7 days (n = 16), or 14 days (n = 1). The remaining 7 studies did not specify the number of days the device was worn. All studies provided the accelerometer or pedometer on the day kinesiophobia was assessed (n = 18). The remaining studies did not specify whether kinesiophobia was measured the day the device was provided or the last day of physical activity assessment (n = 7).”
Reviewer 2 (Discussion): The authors speak about action impulses at several points, or motivational states. Current PA models specify that motivation for movement can be conceptualized as a state, and not just a stable characteristic or trait, as is commonly utilized in the Kinesiophobia literature. Specifically, there are “affectively-charged motivation states”, (ACMS) of which fear is one type. The avoidance motivational construct has also been referred to as “dread”, “aversion” and sometimes “diswant”. It would seem that those with kinesiophobia would have fear states (and thus, active avoidance), which would impair their activity “right now” or in the near term. I suggest exploring some facet of this as future research in the discussion.
Authors: We agree that kinesiophobia is a state that would impair physical activity “right now” or in the near term, which might have influenced the results.
Page 24, lines 509-512: “Because kinesiophobia is a state, i.e., a dynamic psychological variable, the time difference between the physical activity and kinesiophobia assessments, as well as the context of assessment, may have influenced the results.”
Reviewer 2: I suggest exploring more about the sources of fear for physical activity, including fear of injury, fear of falling, fear of the “heart exploding”, fear of hypoglycemic events (very common in Type 1 diabetes). I don’t think that cardiovascular patients having higher kinesiophobia is surprising at all. In my own clinical practice, it seems quite common. Palpitations, angina, arrhythmias, etc. are all very aversive, threatening sensations that most people actively want to avoid, and if experienced in tandem with movement, the movement will be avoided as well.
- Martyn-Nemeth P, Quinn L, Penckofer S, Park C, Hofer V, Burke L. Fear of hypoglycemia: Influence on glycemic variability and self-management behavior in young adults with type 1 diabetes. J Diabetes Complications. 2017;31(4):735-741.
Authors: We agree that exploring the variables that could explain kinesiophobia is of interest. As recommended, they have been added to the Discussion section.
Page 22, lines 462-477: “Our results suggest that patients with a cardiac, neurologic, arthritic, or pulmonary condition, as well as older adults, may be at greater risk for this negative relationship between kinesiophobia and physical activity than those with other conditions. In individuals with a cardiac condition, kinesiophobia and its impact on physical activity may be explained by a fear of inducing a new cardiac event (186) or “causing more damage to the heart” (187), but also by breathlessness (i.e., dyspnea), which reduces the ability to be physically active and damages confidence, leading to persistent anticipation of negative outcomes from physical activity (188). Dyspnea is also a major barrier to physical activity in people with a pulmonary condition, such as chronic obstructive pulmonary disease (COPD) (147). Patients with asthma may have additional disease-related barriers to physical activity, such as the fear of provoking respiratory symptoms and exacerbations (189). Regarding neurologic conditions, chest tightness reported in patients with Parkinson’s disease as a barrier to exercise may be a factor contributing to the association between kinesiophobia and physical activity (190). Another potential factor in these patients (190), as well as in stroke survivors (191) and healthy older adults (192), is fear of falling. In patients with osteoarthritis, the belief that physical activity will “damage the joints” (193) and the perceived fragility of their physical status (194) may be factors contributing to the relationship between kinesiophobia and physical activity.”
Reviewer 2: I suggest that the authors highlight a few prospective study designs that might move the field forward. For instance, does fear or dread (e.g., diswant or aversion) of movement felt or experienced “right now” have any influence on physically active behaviors in the near term (e.g., the next 10 minutes, hour, day)?
Authors: As recommended, we now emphasize the need for prospective studies to move the field forward.
Page 25, lines 536-537: “Particularly, prospective studies are needed to better understand the factors and mechanisms that influence the relationship between kinesiophobia and physical activity.”
Reviewer 2: In Inclusion criteria, I think you meant to add “pedometer” as well.
Authors: Thank you.
Page 7, lines 119-122: “The physical activity measure could be derived from a self-reported measure of the level of physical activity or from a device (e.g., accelerometer, pedometer) worn while participants are engaged in their normal daily activities.”
Reviewer 2: In Data extraction, “Level of..” may need to be reworded. I was imagining categorical variables, but I think you mean continuous.
Authors: We did not see how to change that, so we decided to clarify it in parentheses.
Page 8, lines 149-151: “[…] level of physical activity (continuous or categorical), as well as statistical estimates and significance of the association between kinesiophobia and physical activity.”
Reviewer 2: The statement about this being “emerging research” is not totally accurate. I think the authors demonstrate that there is a wide swath of research in this area. The problem is that it has not been integrated and systematically evaluated.
Authors: Thank you, the adjective “emerging” has been removed.
, posted 27 Sep 2023, validated 29 Sep 2023Dear authors,
Thank you for sumitting your manuscript for evaluation at PCI Health & Mov Sci. I have recieved two helpful and constructive reviews of your submission. As you will see, the reviews are largely positive while also noting several areas for improvement. In particular, I would highlight the need to expand the keyword search to include "fear-avoidance" and the comments regarding timing (i.e., prospective vs. retrospective designs). I request that you go through the reviewers' comments and revise the manuscript to address the points raised. Please resubmit the revised manuscript for further consideration along with a point-by-point response addressing where and how you addressed each comment.
Many thanks and best wishes,
Jasmin Hutchinson
, 23 Sep 2023In the present study, the authors examined the associations between kinesophobia and physical activity outcomes in adults. In my opinion the authors address a relevant question. However, I have highlighted some limitations which dampen my enthusiasm for the manuscript. My greatest concerns with this work were the methodological weaknesses. Author did a great job (thorough analyses, very good graphic representation, sensitivity analyses, data/code sharing…. ) but this review may not be ‘systematic’. Following are some comments based on questions or concerns that arose in my reading. I hope they are useful to the authors.
INTRODUCTION
In my perspective, this section should be revised. Indeed, kinesophobia is presented as an interpersonal determinant of physical activity. However, it’s a PA determinant ‘only’ for people with injuries, chronic pain, fatigue, or illness. In other words, it’s an important factor in clinical context.
Authors suggested that kinesophobia has a major role in dual models. These paragraph could be shortened because kinesophobia is not a major component of these models.
Previous literature reviews about kinesophobia should be presented. Also, the factors tested in the meta-regressions (age, women, pain) should be substantiated in this section.
METHOD
There is an essential limit with the current search strategy. Authors focused exclusively on the “kinesiophobia” word. It is an adapted strategy to identify the studies using TSK. However, the investigations collecting data with the Fear-Avoidance Belief Questionnaire can be published without the kinesophobia word.
After a quick search with FABQ and physical activity’, I identified several not included papers.
PA self-reported questionnaires:
Authors should update their search strategy with more representative key words (e.g., with the name of validated questionnaires). Also, this references of this review should be explored (Effects of Exercise Training on Fear-Avoidance in Pain and Pain-Free Populations: Systematic Review and Meta-analysis). Data collected before the exercise intervention may be useful. Also, physical activity synonyms (e.g., walking) should be added in the search strategy for CINAHL and Psychinfo. In my perspective, SPORTDISCUS database should also be explored.
I don’t understand the following methodological choice : “When a study measured physical activity with both a questionnaire and accelerometers, the correlation included in the analysis was that of the most reliable outcome, i.e., the accelerometer-based outcome.” Associations examined in a same study can be included in a multilevel meta-analysis. Furthermore, a meta-analysis is carried out for PA self-reported measures in your manuscript. Thus, 5 studies are missing in this analysis.
Could you provide more details about this inclusion criteria : “formally test the association between these two variables”. Did you include the studies reporting only an univariate AND OR mutlivariate association (e.g., beta) (see Meta Essentials to manage them [Suurmond R, van Rhee H, Hak T.]).
The current review has been preregistered in Prospero. It is a good point. However, meta-analyses were not planed (e.g., “We do not plan on doing an analysis of subgroups or subsets”) and Risk of bias (quality) assessments were not the tool presented in the manuscript. These gaps should be explained in the current manuscript.
The risk of biais were characterized with the critical appraisal tool for assessing the quality of cross-sectional studies (AXIS). However, there are several randomized controlled trials among included studies (e.g., Priore 2020). They should be assessed with a more specific tool. Additionally, detailed findings for each studies should be provided in supplementary files.
There is a mistake about the I2 in abstract (I2 = 91.8%).
The study design and context of assessment (e.g., clinical, online...) of included investigations should be added in Table 2.
“The remaining 10 authors did not respond to our email.” Authors should provide the references of these 10 papers in supplementary file. As reviewer, I can’t know if you “miss” a paper or authors did not share their data/findings (e.g., doi: 10.2340/16501977-1927).
The global bias-corrected estimate should be also presented in the abstract and added in the table 2.
LIMITS
Kinesophobia is a dynamic psychological variable. Physical exercise interventions or cognitive behavioral therapy can decrease the kinesophobia level. However, you did not “control” the time of assessment. It should be highlighted in Limits.
TSK scales have been criticized because different factor models exist between them (DOI: 10.3109/09593980802662160). These structural differences may influence the findings of the current work.
The question-behavior effect (http://dx.doi.org/10.1037/hea0000104) could underestimate the association between kinesophobia and PA.
Due to weaknesses in methods, I can not interpret the findings of this manuscript.
Paquito BERNARD [In support of 'open science' more broadly, I am signing my reviews]
https://doi.org/10.24072/pci.healthmovsci.100039.rev11Kinesiophobia and Physical Activity: A Systematic Review and Meta-Analysis
I applaud the authors for their rigorous analysis of such an important research topic, which aims to systematically look at the role of fear and aversion of movement on subjective and objective measures of physical activity behavior. I am tempted to accept it as it is; however, I have some major comments for the authors to think about, and a few minor ones as well.
1. First, it is true that these data are highly relevant for dual-process models, which are very popular at this time (example: ART of PA theory). However, they are also highly relevant for other models, such as the Affective Health Behavior Framework (AHBF) (Williams & Evans, 2014; Stevens et al., 2020) and the WANT model of physical activity and sedentarism motivation (Stults-Kolehmainen, et al., 2020). [Note: Dual process models are simply called “dual models” by the authors at least once in the manuscript.]
Williams, D. M., & Evans, D. R. (2014). Current emotion research in health behavior science. Emotion Review, 6(3), 277-287.
Stevens, C. J., Baldwin, A. S., Bryan, A. D., Conner, M., Rhodes, R. E., & Williams, D. M. (2020). Affective determinants of physical activity: a conceptual framework and narrative review. Frontiers in Psychology, 3366.
Stults-Kolehmainen, M. A., Blacutt, M., Bartholomew, J. B., Gilson, T. A., Ash, G. I., McKee, P. C., & Sinha, R. (2020). Motivation states for physical activity and sedentary behavior: desire, urge, wanting, and craving. Frontiers in Psychology, 11, 568390.
2. There seems to be some unexplored temporal issues in the methodologies examined. For instance, the self-report measures are all retrospective (correct?). Were studies looking at PA, that was assessed retrospectively, with measures of Kinesiophobia taken at the same time? Where there any prospective studies with these measures? With objective measures, was the Kinesiophobia measure assessed at the beginning or end? Some measures look at PA that was assessed, perhaps, over a week, two weeks or a month. Do you think this makes any difference? In other words, there could be some influence of memory and reaction to measures of kinesiophobia.
3. The authors speak about action impulses at several points, or motivational states. Current PA models specify that motivation for movement can be conceptualized as a state, and not just a stable characteristic or trait, as is commonly utilized in the Kinesiophobia literature. Specifically, there are “affectively-charged motivation states”, (ACMS) of which fear is one type. The avoidance motivational construct has also been referred to as “dread”, “aversion” and sometimes “diswant”. It would seem that those with kinesiophobia would have fear states (and thus, active avoidance), which would impair their activity “right now” or in the near term. I suggest exploring some facet of this as future research in the discussion.
4. I suggest exploring more about the sources of fear for physical activity, including fear of injury, fear of falling, fear of the “heart exploding”, fear of hypoglycemic events (very common in Type 1 diabetes). I don’t think that cardiovascular patients having higher kinesiophobia is surprising at all. In my own clinical practice, it seems quite common. Palpitations, angina, arrhythmias, etc. are all very aversive, threatening sensations that most people actively want to avoid, and if experienced in tandem with movement, the movement will be avoided as well.
Martyn-Nemeth P, Quinn L, Penckofer S, Park C, Hofer V, Burke L. Fear of hypoglycemia: Influence on glycemic variability and self-management behavior in young adults with type 1 diabetes. J Diabetes Complications. 2017;31(4):735-741.
5. I suggest that the authors highlight a few prospective study designs that might move the field forward. For instance, does fear or dread (e.g., diswant or aversion) of movement felt or experienced “right now” have any influence on physically active behaviors in the near term (e.g., the next 10 minutes, hour, day)?
Minor comments:
1. In Inclusion criteria, I think you meant to add “pedometer” as well.
2. In Data extraction, “Level of..” may need to be reworded. I was imagining categorical variables, but I think you mean continuous.
3. The statement about this being “emerging research” is not totally accurate. I think the authors demonstrate that there is a wide swath of research in this area. The problem is that it has not been integrated and systematically evaluated.
https://doi.org/10.24072/pci.healthmovsci.100039.rev12